
The Brain Shift No One Warned You About: Menopause and the Mind
Menopause has long been framed as a reproductive milestone: the end of periods, the closing of fertility, the body moving into a new phase of life. But that story is incomplete. Increasingly, scientists are recognizing that menopause is not just an ovarian transition. It is also a neurological one.
Modern research in neuroendocrinology suggests that menopause represents a major rewiring of the brain’s energy systems, stress circuitry, and emotional regulation. For many women, the experience is not simply physical—it is cognitive, psychological, and deeply biological. Brain fog, anxiety, disrupted sleep, memory lapses, mood swings: these symptoms are not imagined or exaggerated. They are signs of a brain adapting to a profound hormonal shift.
Menopause Is Not Just Hormonal—It’s Neurological
Estrogen is often described as a “reproductive hormone,” but in reality, it plays a powerful role far beyond fertility. One of its most important functions is in the brain, where it helps regulate energy production, neurotransmitters, and cellular maintenance.
The dominant estrogen during reproductive years—17β-estradiol—acts almost like a metabolic coordinator. It supports the brain’s ability to efficiently use glucose, its primary fuel source. When estrogen levels begin to fluctuate and decline during perimenopause and menopause, the brain does not simply lose a hormone. It loses a stabilizing system.
This is why menopause is increasingly understood as a neuroendocrine transition: a whole-body shift with the brain at its center.
The Brain’s Energy Crisis: Why “Brain Fog” Is Real
The brain is the most energy-demanding organ in the body. Even at rest, it consumes a remarkable share of daily fuel. Estrogen helps neurons meet that demand by promoting glucose uptake and efficient energy metabolism.
When estrogen drops, glucose metabolism becomes less effective. The brain is forced into a kind of metabolic adaptation, searching for alternative sources of energy. Researchers have observed that during menopause, the brain may begin shifting toward ketones and fatty acids as backup fuel.
This adaptation is not inherently harmful—it is a survival mechanism. But it comes at a cost. Some scientists suggest that prolonged energy strain may contribute to structural vulnerability over time, potentially affecting white matter integrity and long-term cognitive resilience.
In mainstream terms: menopause-related brain fog is not a personality flaw or a lack of focus. It is often the brain working harder under a new energy economy.

The Timing Question: Why Hormone Therapy Depends on When
Hormone therapy remains one of the most debated topics in menopause care, and the science has become increasingly nuanced. One of the clearest insights in recent years is that timing matters.
Researchers describe something called the “timing hypothesis.” Starting hormone therapy closer to the final menstrual period—within roughly ten years—may offer supportive effects for brain and cardiovascular health in some women. Starting much later, particularly after age 65, may not provide the same benefits and may carry increased risks.
The reason appears to be cellular. Estrogen supports healthy neurons with strong mitochondrial function. But if brain cells have already entered a more vulnerable metabolic state, reintroducing estrogen may not have the same protective impact.
This does not mean hormone therapy is universally good or bad. It means the brain’s condition and the timing of intervention are critical variables.
Mood Swings Aren’t “Just Emotional”—They’re Neurochemical
One of the most misunderstood aspects of menopause is mood disruption. Irritability, anxiety, sadness, even panic-like symptoms can appear in women with no prior psychiatric history.
While estrogen loss is often blamed, researchers increasingly point to something more specific: hormonal instability. During perimenopause, estrogen levels do not simply decline steadily—they fluctuate unpredictably.
These swings affect the brain’s stress-response system, including serotonin signaling and cortisol regulation. Estrogen normally helps buffer stress by modulating the hypothalamic-pituitary-adrenal axis. When levels become erratic, the brain’s emotional regulation can become more reactive.
For some women, this creates a state of heightened stress sensitivity, where everyday pressures feel biologically amplified.
This is not weakness. It is chemistry. Menopause can temporarily change how the brain processes stress, emotion, and resilience.
Hot Flashes Are Brain Events, Not Just Body Events
Hot flashes are often treated as a surface-level symptom: uncomfortable but temporary. In reality, they are rooted in the brain’s thermoregulatory center.
Vasomotor symptoms reflect the brain struggling to regulate temperature under changing hormonal conditions. And importantly, they are not always short-lived. Large studies show that hot flashes can persist for seven to ten years on average, and longer in some groups.
African American women, for example, experience vasomotor symptoms for a median duration exceeding a decade—nearly twice as long as some Asian populations.
The impact is cumulative. Night sweats disrupt sleep. Sleep disruption worsens cognitive fatigue. Cognitive fatigue worsens mood and stress tolerance. What begins as a “hot flash” often becomes a neurological ripple effect.
Patches vs. Pills: The New Era of Personalized Treatment
Not all hormone therapy is the same, and the route of delivery matters more than many people realize.
Oral estrogen passes through the liver first, which can increase clotting factors and raise the risk of venous thromboembolism in some women. Transdermal estrogen—delivered through patches or gels—bypasses the liver and tends to have a more neutral clotting profile.
The type of progesterone matters too. Micronized progesterone is often considered more physiologically aligned than synthetic progestins, with a potentially improved safety profile for breast and vascular outcomes.
The takeaway is that menopause care is becoming more individualized. The question is no longer simply “hormones or no hormones,” but what formulation, what timing, and what risk profile.
The Social and Economic Cost of Ignoring Menopause
Menopause does not occur in isolation. Cognitive fatigue, sleep disruption, and emotional volatility affect workplaces, families, and relationships.
Researchers estimate significant productivity losses tied to unmanaged menopausal symptoms, including absenteeism and early workforce attrition. Beyond economics, menopause-related neurochemical strain can quietly reshape interpersonal dynamics.
When sleep is fragmented and stress reactivity rises, emotional buffering decreases. Midlife relationship strain is often interpreted as purely social, but biology plays an underrecognized role.
Supporting menopausal brain health is not just a medical issue—it is a societal one.
The Future: Beyond Decline, Toward Brain Longevity
New therapies are emerging that aim to treat menopause with greater selectivity and fewer systemic risks. One promising candidate is estetrol, a naturally occurring estrogen produced during pregnancy, now being studied for symptom relief with a refined safety profile.
But the larger shift is conceptual. Menopause is not simply an ending. It is a transition—one that the brain must metabolically navigate.
If we stop treating menopause as inevitable decline and begin understanding it as a neurological adaptation, we can offer women something better than dismissal or silence. We can offer informed care, metabolic support, emotional validation, and long-term brain health strategies.
Menopause does not mean the brain is failing. It means the brain is changing. And with the right support, that change can be navigated with strength, clarity, and longevity.
Neurobiological, Bioenergetic, and Sociosystemic Analysis of the Menopausal Transition
The Cardiovascular- Neuroendocrine Metamorphosis and the Bioenergetic Crisis of the Aging Female
The menopausal transition is not simply a local shutdown of reproductive function; it is a far-reaching neuroendocrine reconfiguration marked by declining levels and unpredictable oscillations of ovarian steroids. [1] For the female brain, this shift functions like a metabolic “reset.” Estrogen—especially 17β-estradiol (E2)—acts as a central coordinator of cerebral bioenergetics, helping meet the brain’s constant energy requirements for synaptic activity and cognitive robustness. [2] In hippocampal and cortical neurons, estrogen-driven signaling is tightly coupled to the preservation of aerobic glycolysis and oxidative phosphorylation. [2] By supporting ATP production through citric-acid-cycle flux and by promoting glucose availability (including upregulation of transporters such as GLUT1), E2 helps keep glucose as the dominant fuel used by the central nervous system. [2]
As women near 57 years of age—often several years after menopause—glucose utilization in the brain can be measurably diminished after prolonged loss of estrogen’s regulatory effects. [3] The result is a sustained bioenergetic strain. Evidence supports an early, possibly contributory role for mitochondrial dysfunction and brain hypometabolism in the cascade that leads to Alzheimer’s disease (AD) pathology. [3, 4, 5] When glucose metabolism becomes insufficient, the brain compensates by shifting toward alternative energy pathways: first relying more heavily on ketone-based metabolism and, with progression, moving further into fatty acid oxidation (FAO). [4, 5] This adaptation carries risk; FAO has been linked to white matter injury and increased ketone-body burden. [4, 5] In effect, the brain may begin to consume endogenous lipid stores—particularly myelin in white matter—to maintain energy supply, promoting deterioration of connectivity and circuit integrity. [4, 5]
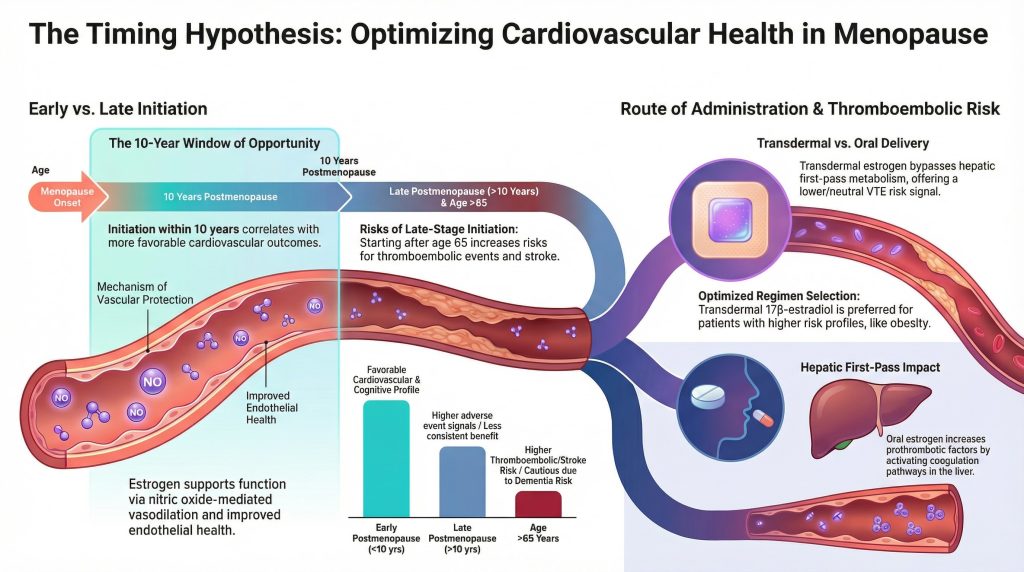
Table 1. Comparative Bioenergetic Parameters Across the Menopausal Transition
| Bioenergetic Parameter | Estrogen-Rich State (Premenopause) | Estrogen-Depleted State (Postmenopause) | Implications for Neurodegeneration |
| Primary fuel source | Glucose (aerobic glycolysis) [2] | Ketone bodies / fatty acids [4, 5] | Higher amyloid vulnerability; white matter loss [4, 5] |
| ATP generation efficiency | Optimized via TCA/OXPHOS [2] | Reduced; mitochondrial hypofunction [4, 5] | Lower neuronal stress tolerance [4, 5] |
| Calcium homeostasis | Maintained; anti-excitotoxic [2] | Dysregulated vulnerability [6] | Cell death in metabolically stressed neurons [4, 5] |
| Antioxidant defense | Enhanced; ROS buffering [2] | Diminished; oxidative stress [3, 4] | Mitochondrial injury, glial activation [3] |
| Cholesterol trafficking | Efficient transport/clearance [5] | Impaired; plaque-associated pathways [5] | Lipid catabolism and myelin breakdown [4, 5] |
The “healthy cell bias of estrogen action” model proposes that hormone therapy benefits depend on the biologic condition of the neural system at the time estrogen is introduced. [2, 4] In metabolically intact neurons, estrogen tends to support homeostasis and antioxidant capacity; however, when the system is already in a degenerative or hypometabolic state, estrogen can intensify injury by increasing energetic demand on dysregulated pathways. [2, 4] Timing therefore matters for a 57-year-old: initiation of therapy within roughly ten years of the final menstrual period (FMP) is more often associated with favorable cardiometabolic and cognitive risk patterns, while later initiation may provide less benefit. [6, 7, 8]
Affective Regulation and the Window of Vulnerability to Stress
The menopause transition is widely described as a “window of vulnerability” for new or worsening depressive symptoms, anxiety, and irritability. [9, 10] For a 57-year-old woman reporting heightened anxiety and irritability after a major stressor two years earlier, a key mechanism is the intersection of estrogen withdrawal with serotonergic regulation and steroid-linked mood circuitry. [1, 11] Serotonin neurons in the midbrain raphe express estrogen receptor beta and progestin receptors, making them direct targets of ovarian steroids. [11] Estrogen supports serotonergic function in part by regulating synthesis-related pathways (including TPH2-linked mechanisms) and stress responsivity. [11] When estrogen levels fall—or fluctuate sharply—the serotonin system can become more stress-reactive, often presenting clinically as irritability and reduced coping capacity. [11]
The “Estradiol Withdrawal Hypothesis” emphasizes that rapid physiologic shifts, not only low absolute hormone levels, can destabilize mood. [12, 13] Experimental crossover designs show that women with a history of perimenopausal depression (PMD) can experience clinically meaningful symptom recurrence when switched from estradiol to placebo, whereas women without such histories often remain stable under the same manipulation. [12] This pattern supports hormone-flux sensitivity in a biologically susceptible subgroup. [13, 14] For the patient in question, the major stress event two years prior—potentially near the time of her FMP—may have served as an amplifying trigger in a system already sensitized by fluctuating hormones. [13, 14]

Table 2. Risk Factors for Affective Disorders During the Menopausal Transition
| Factor | Association with Menopausal Depression/Anxiety | Risk Ratio / Odds Ratio (as reported) |
| History of depression | Strongest predictor of new/recurrent episodes [9, 10] | Often ~OR 2–5 (varies by cohort) [9] |
| Menopausal status | Perimenopause vs premenopause increases risk [9, 10] | Often ~OR ~2 (varies by definition) [9] |
| Hormone variability | Rapid fluctuations in E2/FSH predict symptoms [13, 14] | Predictive association in longitudinal work [13, 14] |
| Life stressors | Trauma/strain/lack of support modulate risk [13, 14] | Strong interaction effects [13, 14] |
| Vasomotor symptoms | VMS burden linked to sleep/mood decline [1, 15] | Correlational + bidirectional models [15] |
Furthermore, ovarian hormones modulate the hypothalamic-pituitary-adrenal (HPA) axis, which governs the stress response. [11] Estrogen typically facilitates a more regulated stress response; withdrawal can increase stress reactivity and alter cortisol feedback sensitivity. [11] Chronic stress combined with low estrogen may reduce physiologic buffering capacity, plausibly worsening irritability and anxiety in vulnerable patients. [11] For a woman at age 57 whose symptoms intensified after a major stressor at age 55, the clinical picture is consistent with an unregulated stress response compounded by postmenopausal neurochemical and metabolic shifts. [11]
Estrogen Receptor Signaling and Neuroplasticity
Estrogens exert their effects through genomic and non-genomic signaling mediated by estrogen receptor pathways in brain regions critical for memory and emotional regulation (hippocampus, prefrontal cortex). [1, 2, 16] 17β-estradiol (E2) is the predominant and most potent estrogen during reproductive years, while estrone (E1) becomes relatively more prominent after menopause due to peripheral conversion. [1] Estradiol supports neuroplasticity via pathways linked to synaptic maintenance and neurotrophin signaling (including BDNF-associated effects). [2, 16]
Evidence suggests that E2-based approaches may be more consistently aligned with cognitive and mood support than E1-heavy formulations. [6, 7] The density and sensitivity of estrogen signaling systems may shift during the transition, and subjective memory complaints and mood lability are common clinical correlates. [16, 17]
Table 3. Estrogen Variants and Their Impact on Neural Health
| Estrogen Type | Primary Biological Source | Effect on Neuroplasticity | Clinical Notes |
| 17β-Estradiol (E2) | Ovarian follicles; local brain [1, 2] | Supports synaptic function [2, 16] | Used in many MHT; route matters [7] |
| Estrone (E1) | Peripheral adipose conversion [1] | Less consistent benefit vs E2 [6, 17] | Dominant postmenopause fraction [1] |
| Estetrol (E4) | Fetal liver–derived [18] | Selective tissue profile; evolving [18, 19] | E4COMFORT design published [19] |
Vasomotor Symptom Trajectories and Racial Disparities
Vasomotor symptoms (VMS), such as hot flashes and night sweats, arise from hypothalamic thermoregulatory zone narrowing in the context of estrogen withdrawal. [1, 15] Large cohort findings indicate that frequent VMS can persist for many years, with meaningful racial and ethnic disparities in symptom duration and post-FMP persistence. [20]

Table 4. Duration of Vasomotor Symptoms by Racial and Ethnic Group (Cohort Findings)
| Racial/Ethnic Group | Median VMS Duration (years) | Median Post-FMP Persistence (years) |
| African American | 10.1 [20] | 6.0 [20] |
| Hispanic | 8.9 [20] | 6.4 [20] |
| White (Non-Hispanic) | 6.5 [20] | 4.6 [20] |
| Chinese | 5.4 [20] | 3.5 [20] |
| Japanese | 4.8 [20] | 3.3 [20] |
Cardiovascular Health and the Timing Hypothesis
Cardiovascular disease (CVD) incidence rises sharply after menopause. [1] Estrogen supports vascular function in part via nitric oxide–mediated vasodilation and effects on endothelial function. [8] The “timing hypothesis” suggests that menopausal hormone therapy initiated in women younger than 60 or within 10 years of menopause onset is less likely to increase CVD risk and may be associated with more favorable outcomes than later initiation. [7, 8]
Initiating therapy later (eg, >10 years postmenopause or after age 65) is more consistently associated with thromboembolic and stroke risks, in part because established vascular pathology may be less responsive to estrogen’s protective mechanisms. [7, 8] For a 57-year-old woman, initiating treatment generally remains within the favorable window when indicated and when risk screening is appropriate. [7, 8]
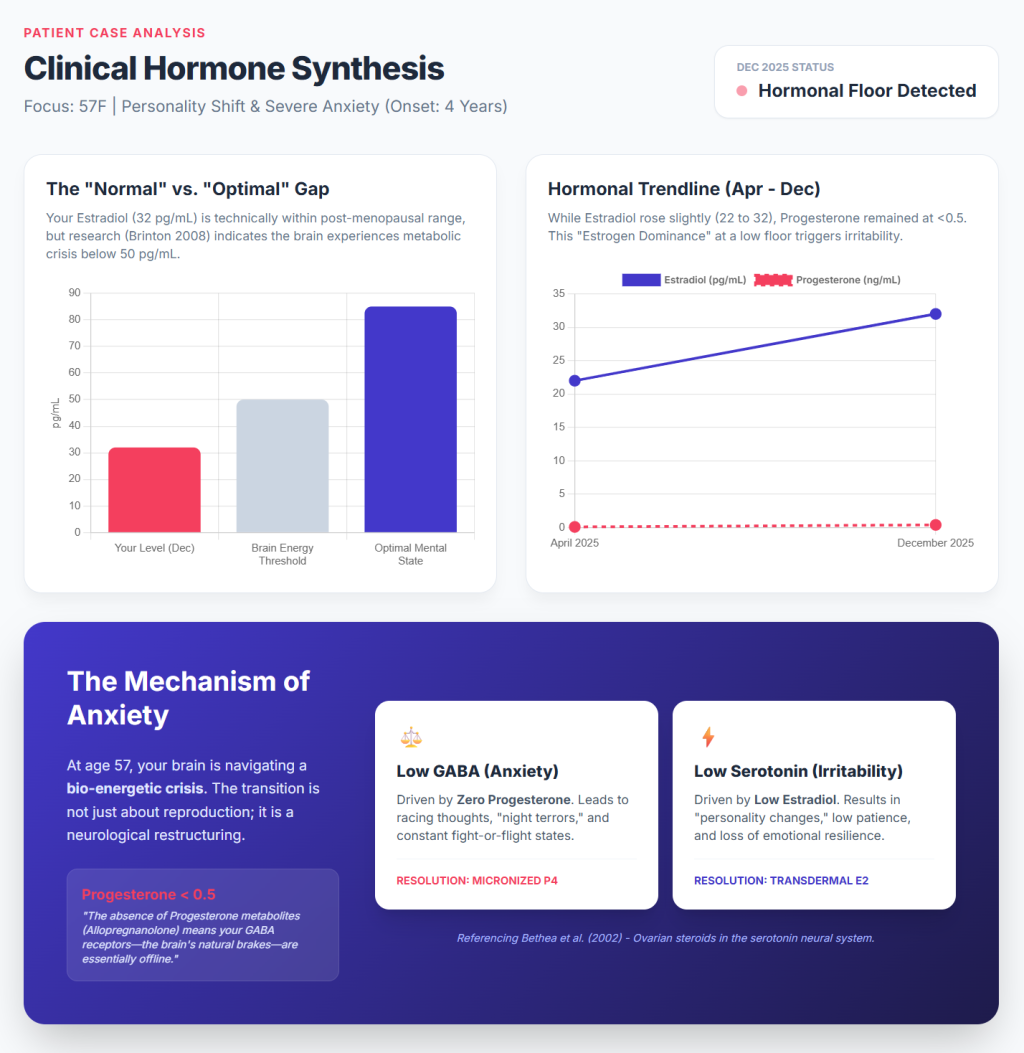
Table 5. Cardiovascular and Cognitive Outcomes by HRT Initiation Timing
| Timing Window | Cardiovascular Effect | Cognitive / AD Risk Effect |
| Early postmenopause (<10 yrs) | More favorable profile [7, 8] | Potentially more favorable framing [6, 17] |
| Late postmenopause (>10 yrs) | Higher adverse event signals [7, 8] | Less consistent benefit; cautious [7, 17] |
| Age >65 years | Higher thromboembolic risk [7, 8] | Dementia risk signals in late start [7] |
Thromboembolic Risk and the Route of Administration
One of the most significant safety considerations in prescribing hormone therapy is venous thromboembolism (VTE). Oral estrogen undergoes hepatic first-pass metabolism, increasing prothrombotic factors and activating coagulation pathways. [21] Observational and clinical data show oral regimens are associated with increased VTE risk. [21, 22]
In contrast, transdermal estrogen bypasses hepatic first-pass metabolism and is associated with lower or neutral VTE risk signals in comparative analyses. [22] For women with risk factors such as obesity or smoking history, transdermal estrogen is commonly preferred when hormone therapy is indicated. [7, 22]
Table 6. VTE Risk by Regimen and Route (Comparative Evidence)
| HT Regimen | VTE Association | Evidence Notes |
| Oral estrogen (general) | Increased VTE risk [21, 22] | Risk varies by formulation and population [21, 22] |
| Transdermal estrogen | Lower/neutral risk vs oral [22] | Preferred in higher-risk profiles [7, 22] |
| Progestogen effects | Progestogen choice matters [23] | Micronized progesterone often favored [23] |

Oncological Perspectives: Re-evaluating Breast Cancer Risk
The 2002 Women’s Health Initiative (WHI) report significantly influenced clinical practice by identifying increased invasive breast cancer risk with combined estrogen (CEE) and medroxyprogesterone acetate (MPA). [24] Long-term follow-up added nuance: among women with hysterectomy randomized to estrogen alone, breast cancer incidence and mortality were lower than placebo in extended analyses. [25]
Across studies, risk appears to be driven substantially by the progestogen component, particularly synthetic progestins. [23] Micronized progesterone is often preferred in contemporary practice discussions because comparative evidence suggests more favorable risk profiles relative to certain synthetic progestins, with potential sleep-related benefits. [7, 23]
The Role of Androgens and Testosterone Therapy
Testosterone is a crucial hormone in female physiology, and androgen levels decline with age and menopause stage. [26] Physiologic-dose testosterone has evidence-based benefit for hypoactive sexual desire disorder (HSDD) and may improve sexual function without virilization when appropriately dosed and monitored. [26] Some clinical literature and expert discussion also report benefits in energy and well-being in selected patients, though indications beyond HSDD require careful risk-benefit framing. [26, 27]
Table 7. Testosterone in Women: Common Myths vs Evidence
| Common Myth | Clinical Reality / Evidence |
| “Testosterone is only for men” | Consensus recognizes therapy primarily for HSDD [26] |
| “It causes masculinization” | Low-dose regimens minimize virilization risk [26] |
| “It increases aggression” | No routine aggression increase at physiologic doses [26] |
| “It’s only for libido” | Primary supported indication is HSDD [26, 27] |
| “It causes liver damage” | Non-oral approaches avoid first-pass issues [26] |
Socioeconomic Position, Workforce, and Interpersonal Dynamics
The age at natural menopause reflects interactions among genetics, exposures, and socioeconomic position. [28] Higher educational attainment is associated with later menopause, while socioeconomic adversity is linked to earlier onset. [28] This transition occurs during peak professional years, where RAND estimates substantial annual productivity losses attributable to symptoms. [29] Furthermore, menopausal symptoms can affect interpersonal dynamics; divorce rates among adults over 50 have risen substantially since 1990, with women initiating a majority of these divorces. [30]

Next-Generation Estrogen: Estetrol (E4)
Estetrol (E4) is a naturally occurring estrogen produced by the fetal liver and developed as a therapeutic candidate with selective tissue activity. [18] The E4COMFORT I and II trial design has been published in Maturitas (January 2026), evaluating E4 15 mg and 20 mg for reduction in moderate-to-severe VMS, with long-term safety evaluation including endometrial safety. [19] ClinicalTrials registration includes NCT04209543 and NCT04090957. [19]
Clinical Synthesis: Managing the 57-Year-Old Patient
For a 57-year-old postmenopausal woman experiencing increased irritability and anxiety following a significant stress event, the therapeutic goal is to restore neuroendocrine stability while minimizing risks. [7, 8] Her symptom pattern fits a plausible interaction between hormone variability, serotonergic stress vulnerability, and HPA-axis dysregulation. [13, 14, 11]
Recommended Assessment and Treatment Hierarchy
- Determine stage and severity: Quantify irritability/anxiety impact on quality of life and identify alignment with the “window of vulnerability.” [1, 9, 10]
- Establish baseline risks: Evaluate cardiovascular markers, breast cancer risk, and VTE profile. [7, 21, 22]
- Select optimized HT regimen: Prefer transdermal 17β-estradiol and micronized progesterone to minimize VTE and oncological risk signals. [7, 22, 23]
- Integrative support: Address behavioral interventions that improve sleep and support stress resilience, given the coupling between sleep disruption and mood. [1, 15]



References
- Santoro N, Epperson CN, Mathews SB. Menopausal Symptoms and Their Management. Endocrinol Metab Clin North Am. 2015;44(3):497-515. doi:10.1016/j.ecl.2015.05.001
- Rettberg JR, Yao J, Brinton RD. Estrogen: a master regulator of bioenergetic systems in the brain and body. Front Neuroendocrinol. 2014;35(1):8-30. doi:10.1016/j.yfrne.2013.08.001
- Mosconi L, Berti V, Quinn C, et al. Sex differences in Alzheimer risk: Brain imaging of endocrine vs chronologic aging. Neurology. 2017;89(13):1382-1390. doi:10.1212/WNL.0000000000004425
- Yao J, Brinton RD. Estrogen regulation of mitochondrial bioenergetics: implications for prevention of Alzheimer’s disease. Adv Pharmacol. 2012;64:327-371. doi:10.1016/B978-0-12-394816-8.00010-6
- Adlimoghaddam A, Fontaine KM, Albensi BC. Age- and sex-associated alterations in hypothalamic mitochondrial bioenergetics and inflammatory-associated signaling in the 3xTg mouse model of Alzheimer’s disease. Biol Sex Differ. 2024;15(1):95. Published 2024 Nov 25. doi:10.1186/s13293-024-00671-7
- Sochocka M, Karska J, Pszczołowska M, et al. Cognitive Decline in Early and Premature Menopause. Int J Mol Sci. 2023;24(7):6566. Published 2023 Mar 31. doi:10.3390/ijms24076566
- “The 2022 Hormone Therapy Position Statement of The North American Menopause Society” Advisory Panel. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause. 2022;29(7):767-794. doi:10.1097/GME.0000000000002028
- El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement From the American Heart Association. Circulation. 2020;142(25):e506-e532. doi:10.1161/CIR.0000000000000912
- Maki PM, Kornstein SG, Joffe H, et al. Guidelines for the Evaluation and Treatment of Perimenopausal Depression: Summary and Recommendations. J Womens Health (Larchmt). 2019;28(2):117-134. doi:10.1089/jwh.2018.27099.mensocrec
- Kulkarni J, Gurvich C, Mu E, et al. Menopause depression: Under recognised and poorly treated. Aust N Z J Psychiatry. 2024;58(8):636-640. doi:10.1177/00048674241253944
- Rubinow DR, Schmidt PJ. Gonadal steroid regulation of mood: the lessons of premenstrual syndrome. Front Neuroendocrinol. 2006;27(2):210-216. doi:10.1016/j.yfrne.2006.02.003
- Schmidt PJ, Ben Dor R, Martinez PE, et al. Effects of Estradiol Withdrawal on Mood in Women With Past Perimenopausal Depression: A Randomized Clinical Trial. JAMA Psychiatry. 2015;72(7):714-726. doi:10.1001/jamapsychiatry.2015.0111
- Gordon JL, Rubinow DR, Eisenlohr-Moul TA, Leserman J, Girdler SS. Estradiol variability, stressful life events, and the emergence of depressive symptomatology during the menopausal transition. Menopause. 2016;23(3):257-266. doi:10.1097/GME.0000000000000528
- Miller VM, Kling JM, Files JA, et al. What’s in a name: are menopausal “hot flashes” a symptom of menopause or a manifestation of neurovascular dysregulation?. Menopause. 2018;25(6):700-703. doi:10.1097/GME.0000000000001065
- Thurston RC, Joffe H. Vasomotor symptoms and menopause: findings from the Study of Women’s Health across the Nation. Obstet Gynecol Clin North Am. 2011;38(3):489-501. doi:10.1016/j.ogc.2011.05.006
- Greendale GA, Derby CA, Maki PM. Perimenopause and cognition. Obstet Gynecol Clin North Am. 2011;38(3):519-535. doi:10.1016/j.ogc.2011.05.007
- Russell JK, Jones CK, Newhouse PA. The Role of Estrogen in Brain and Cognitive Aging. Neurotherapeutics. 2019;16(3):649-665. doi:10.1007/s13311-019-00766-9
- Coelingh Bennink HJT, Gosden R, Stanczyk FZ, Adashi EY. The rediscovery of estetrol and its implications for estrogen treatment. Menopause. 2025;32(7):648-651. Published 2025 Jul 1. doi:10.1097/GME.0000000000002537
- Panay N, Simoncini T, Taziaux M, et al. Estetrol for the treatment of moderate to severe vasomotor symptoms in postmenopausal women: The design of the E4COMFORT I and II trials. Maturitas. 2026;204:108781. doi:10.1016/j.maturitas.2025.108781
- Avis NE, Crawford SL, Greendale G, et al. Duration of menopausal vasomotor symptoms over the menopause transition. JAMA Intern Med. 2015;175(4):531-539. doi:10.1001/jamainternmed.2014.8063
- Canonico M, Plu-Bureau G, Lowe GD, Scarabin PY. Hormone replacement therapy and risk of venous thromboembolism in postmenopausal women: systematic review and meta-analysis. BMJ. 2008;336(7655):1227-1231. doi:10.1136/bmj.39555.441944.BE
- Vinogradova Y, Coupland C, Hippisley-Cox J. Use of hormone replacement therapy and risk of venous thromboembolism: nested case-control studies using the QResearch and CPRD databases. BMJ. 2019;364:k4810. Published 2019 Jan 9. doi:10.1136/bmj.k4810
- Scarabin PY. Progestogens and venous thromboembolism in menopausal women: an updated oral versus transdermal estrogen meta-analysis. Climacteric. 2018;21(4):341-345. doi:10.1080/13697137.2018.1446931
- Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA. 2002;288(3):321-333. doi:10.1001/jama.288.3.321
- Chlebowski RT, Rohan TE, Manson JE, et al. Breast Cancer After Use of Estrogen Plus Progestin and Estrogen Alone: Analyses of Data From 2 Women’s Health Initiative Randomized Clinical Trials. JAMA Oncol. 2015;1(3):296-305. doi:10.1001/jamaoncol.2015.0494
- Davis SR, Baber R, Panay N, et al. Global Consensus Position Statement on the Use of Testosterone Therapy for Women. J Clin Endocrinol Metab. 2019;104(10):4660-4666. doi:10.1210/jc.2019-01603
- Glaser R, Dimitrakakis C. Testosterone therapy in women: myths and misconceptions. Maturitas. 2013;74(3):230-234. doi:10.1016/j.maturitas.2013.01.003
- Schoenaker DA, Jackson CA, Rowlands JV, Mishra GD. Socioeconomic position, lifestyle factors and age at natural menopause: a systematic review and meta-analyses of studies across six continents. Int J Epidemiol. 2014;43(5):1542-1562. doi:10.1093/ije/dyu094
- RAND Corporation. The Economic Impacts of Menopause in the United States. 2022. https://www.rand.org/content/dam/rand/pubs/research_reports/RRA4200/RRA4292-1/RAND_RRA4292-1.pdf
- Brown SL, Lin IF. The gray divorce revolution: rising divorce among middle-aged and older adults, 1990-2010. J Gerontol B Psychol Sci Soc Sci. 2012;67(6):731-741. doi:10.1093/geronb/gbs089